
There is a habit, understandable but risky, of treating a drug’s headline number as its starting point. With tirzepatide, that habit causes most of the trouble people report. The medication is not meant to begin at the dose that produced the widely quoted weight-loss figures. It is meant to begin low and rise slowly, on a fixed schedule, and the schedule itself is part of what makes the drug tolerable. This piece lays out how that schedule is built, what the evidence actually measured, and what a person on the medication should be keeping track of along the way.
Escalation is the mechanism, not a formality
Tirzepatide is a once-weekly injection, and its dosing is structured as a deliberate, stepwise increase over time. A person starts at a low dose and moves up at set intervals, and that pacing exists specifically to limit side effects [P2]. It is not caution added on top of the treatment. It is the treatment, as designed.
The reason the ramp matters becomes clear once you know what the common side effects are: nausea, diarrhea, vomiting, and constipation, clustering most heavily around each dose increase [P2]. A slow climb gives the body room to adjust at each step before the next one arrives, and that adjustment period is what keeps those symptoms manageable for the majority of people who take the drug. When someone reports that a GLP-1 medication was intolerable, one of the first useful questions is whether the dose rose faster than intended. The schedule is the safeguard. It works best when it is respected rather than rushed.
It follows that anyone picturing the biggest results in the first weeks should set that picture aside. The strongest effects sit at the top of a ladder a person climbs deliberately, not at its base.
What the trial actually measured
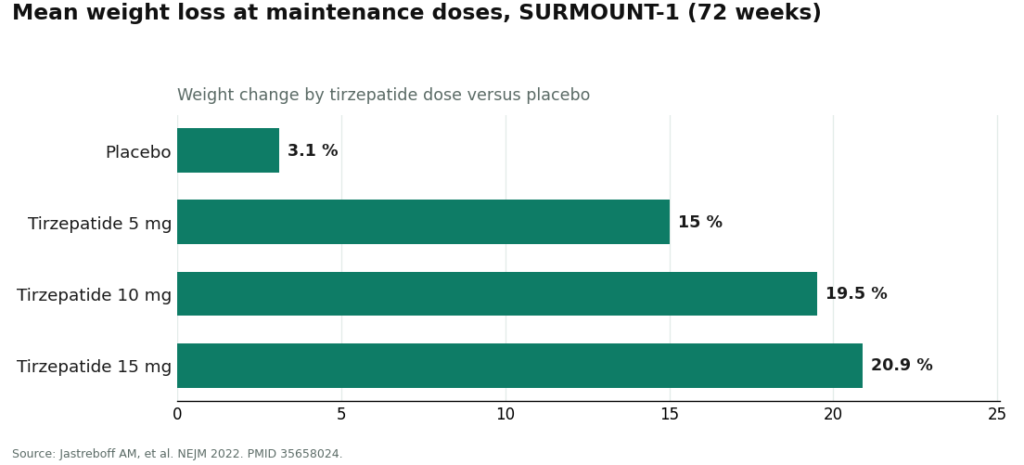
Connecting the dose levels to the evidence removes some of the mystery from the schedule. In SURMOUNT-1, the pivotal obesity trial published in the New England Journal of Medicine, adults were maintained at higher doses and followed for 72 weeks. Average weight loss came to roughly 15.0% at the 5 mg dose, 19.5% at 10 mg, and 20.9% at 15 mg, compared with about 3.1% on placebo [P1].
Those figures describe outcomes at maintenance doses reached after escalation, not outcomes at the start of treatment. The 5 mg, 10 mg, and 15 mg numbers sit near the top of the ladder; the low starting dose does not appear in that list at all, because its purpose is tolerability rather than peak effect. Both things are true at once: the results are genuine, and they belong to doses a person builds toward, not doses a person begins on.
It is also worth remembering what kind of number an average is. These figures come from a trial in which the medication was paired with lifestyle counseling, and they describe a group, not a guarantee to any one person. They are useful for understanding what each dose is for. They are not a promise attached to any individual’s chart.
Why the stomach is where this shows up
A short detour into mechanism explains the pattern above. Tirzepatide is a dual agonist, activating both the GLP-1 receptor and the GIP receptor; structurally, it is a 39-amino-acid analog of GIP [P3]. Engaging those two pathways increases insulin release in a glucose-dependent way, slows gastric emptying, and reduces appetite [P3].
That slowed gastric emptying is the same mechanism behind both the fullness patients want and the nausea they generally do not. It is precisely why the dose rises gradually: the gut needs time to adapt to an increasingly strong signal. Framed this way, early digestive discomfort reads less like a failure and more like an expected edge of a mechanism doing its job, provided the climb is not rushed past what the body can absorb.
The record that makes dosing decisions possible
A dose is a number on a pen. What turns that number into good clinical decision-making is the record kept alongside it, and this is where people most often shortchange themselves. Arriving at a check-in with a general impression that “things seem fine” gives a prescriber little to work with. Arriving with an actual log changes the conversation.
Worth tracking, every week:
- The dose taken and the date. Escalation runs on a schedule, and the schedule only functions if both patient and prescriber know exactly where things stand on it.
- Side effects and their severity. Note when nausea or digestive changes appear, and whether they are easing as the body settles at a given dose. This is often the single most useful input for deciding whether to hold a dose a while longer before stepping up.
- The weight trend across weeks, not the daily number. Day-to-day weight fluctuates for reasons unrelated to the drug. The trend across weeks is the signal, and it is what the trial itself measured.
- Anything resembling a warning sign. Severe or persistent abdominal pain in particular is something the label associates with pancreatitis risk, and it warrants a prompt call to a clinician rather than a note in a log to revisit later [P2].
None of this requires anything elaborate, though a dedicated tool helps consistency. Patients enrolled in a supervised program can use the FormBlends tracker app to log weekly dose and symptoms, arriving at appointments with a real record instead of a hazy recollection. To be precise about what that tool is: a logging aid, not a prescription and not a checkout. The discipline of writing things down is the point, because a real record is what turns “how’s it going” into an actual clinical decision.
Three ways this goes wrong
Rushing the ladder. This is the most common self-inflicted problem. Impatience at a low dose leads to stepping up faster than intended, running directly into the side effects the schedule was built to soften. Each rung is meant to be given time.
Mistaking the headline dose for the starting dose. The 15 mg figure attached to the largest weight-loss number is a place a person arrives at, not a place a person begins [P1] [P2]. Starting high maximizes side effects, not results.
Dosing without a screen or a record. This is the mistake specific to unsupervised access, and it is the one with the highest stakes. Tirzepatide carries the FDA’s most serious warning, a boxed warning, for thyroid C-cell tumors, and it is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 [P2]. There is also a documented interaction in which tirzepatide can reduce how well oral contraceptives work, which is why the label recommends adding a barrier method or switching to a non-oral method for four weeks after starting and after each dose increase [P2]. A schedule a person sets for themselves from a vial that arrives in the mail, with no one checking for these things beforehand, skips every one of those safeguards. The dosing ladder is a clinical tool, and it functions best inside a relationship where someone has screened the patient first and can adjust the pace based on how that patient actually responds.
What supervised dosing looks like, described plainly
The structure the label assumes looks like this: a licensed clinician evaluates the patient and checks for the contraindications described above, a prescription is written where appropriate, and a licensed pharmacy dispenses the medication, with follow-up that actually makes use of the record the patient has kept. A licensed telehealth provider such as FormBlends is organized around that structure. That is offered here as a description of what supervised dosing entails, nothing more. There is no scorecard implied, and nothing here to click through.
The short version
Start low. Climb slowly. The 15.0%, 19.5%, and 20.9% figures are maintenance-dose results reached after escalation, not opening numbers [P1]. Expect gastrointestinal side effects mainly around dose increases, and let the schedule do the work of softening them [P2]. Keep a weekly record of dose, symptoms, and weight trend so the next dosing decision rests on information rather than guesswork. And get screened before starting, since the boxed-warning contraindication and the contraceptive interaction are exactly the sort of thing a self-directed plan tends to miss [P2]. Handled properly, inside a supervised structure, the strong trial numbers have a genuine chance of applying to the person taking the drug, not just the population that was studied.
Honest answers to common questions
What is the starting dose, and why isn’t it the dose behind the big numbers? The opening dose is low and taken once weekly, set deliberately below the maintenance doses that produced the widely cited results. Its job is tolerability, giving the gut time to adjust before the signal intensifies. The 15.0%, 19.5%, and 20.9% figures belong to doses reached over weeks of escalation, not to the first injection [P1].
How quickly can the dose be raised? Increases happen on a fixed schedule at set intervals, not on a whim, and the spacing exists so each step has time to settle [P2]. If side effects are still uncomfortable when an increase is due, holding at the current dose a while longer is a normal, reasonable adjustment, and one that is easier to justify with a written record of how each dose actually felt.
Why do gastrointestinal side effects worsen with each increase? Tirzepatide slows gastric emptying, and that single effect produces both the fullness that is wanted and the nausea that is not [P3]. Every dose increase asks the gut to adapt to a stronger version of that signal, which is when nausea, diarrhea, vomiting, and constipation tend to appear together [P2]. A slow climb is what keeps that adjustment manageable for most people.
What should be tracked each week while escalating? The dose and date, side effects and their severity, weight trend across weeks rather than single days, and anything resembling a warning sign. Severe or persistent abdominal pain deserves prompt attention, given its association with pancreatitis on the label [P2]. A genuine record turns a vague check-in into a decision a prescriber can actually act on.
Who shouldn’t take tirzepatide? Anyone with a personal or family history of medullary thyroid carcinoma or MEN 2 is contraindicated, given the boxed warning for thyroid C-cell tumors [P2]. The drug can also reduce the effectiveness of oral contraceptives, so the label calls for a barrier method or a non-oral method for four weeks after starting and after each increase [P2]. These are exactly the checks that go missing when medication arrives unsupervised, by mail, with no clinician involved.
What is tirzepatide, in mechanistic terms?
Tirzepatide is a once-weekly injectable that activates two gut hormone receptors at once, GIP and GLP-1, which is why it’s described as a dual agonist. Those hormones slow gastric emptying, reduce appetite, and help the body regulate blood sugar. Most single-target GLP-1 drugs only engage one of those receptors, so the dual mechanism is a genuine pharmacological difference, not a marketing distinction.
Does the weight loss hold up, or is it overstated?
The trial results are real. In the SURMOUNT program, participants on the highest dose lost around 20 percent of body weight on average over roughly 72 weeks, more than earlier GLP-1 medications achieved in comparable trials. Averages, though, conceal a wide range: some people lose considerably more, some considerably less, and outcomes depend heavily on dose tolerance, diet, and how long a person stays on treatment.
How does tirzepatide compare with semaglutide?
In trials published so far, tirzepatide has generally produced larger average weight loss than semaglutide, though head-to-head comparison studies remain limited. Side effect profiles look similar, mostly nausea, constipation, and fatigue during dose increases. Cost, insurance coverage, and individual response vary enough that which drug is “better” genuinely differs from person to person, a conversation worth having with a prescriber rather than settling from a chart alone.
Are Mounjaro and Zepbound the same drug?
Both contain tirzepatide; the difference is the approved indication. Mounjaro is approved for type 2 diabetes, Zepbound for chronic weight management. Calling tirzepatide simply a GLP-1 is only half accurate: it activates the GLP-1 receptor, but also the GIP receptor, making “dual GIP/GLP-1 agonist” the more precise term. Patients accessing tirzepatide through a physician-supervised compounding pharmacy such as FormBlends are receiving the same active ingredient outside branded packaging.
References
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. New England Journal of Medicine, 2022. PMID 35658024. Mean weight change at 72 weeks roughly 15.0% (5 mg), 19.5% (10 mg), and 20.9% (15 mg) versus 3.1% placebo at maintenance doses, treatment-regimen estimand. https://www.nejm.org/doi/full/10.1056/NEJMoa2206038
- Tirzepatide (Zepbound) FDA-approved label, DailyMed. Once-weekly dosing with gradual dose escalation to limit gastrointestinal adverse reactions; boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2; acute pancreatitis warning; oral hormonal contraceptive interaction with advice to add a barrier method or switch to a non-oral method for 4 weeks. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=487cd7e7-434c-4925-99fa-aa80b1cc776b
- Farzam K, Patel P. Tirzepatide. StatPearls, NCBI Bookshelf. Dual GIP and GLP-1 receptor agonist, 39-amino-acid GIP analog; increases glucose-dependent insulin secretion, slows gastric emptying, reduces appetite.



